Understanding Primary Hyperaldosteronism: Causes, Symptoms, and Treatment Options
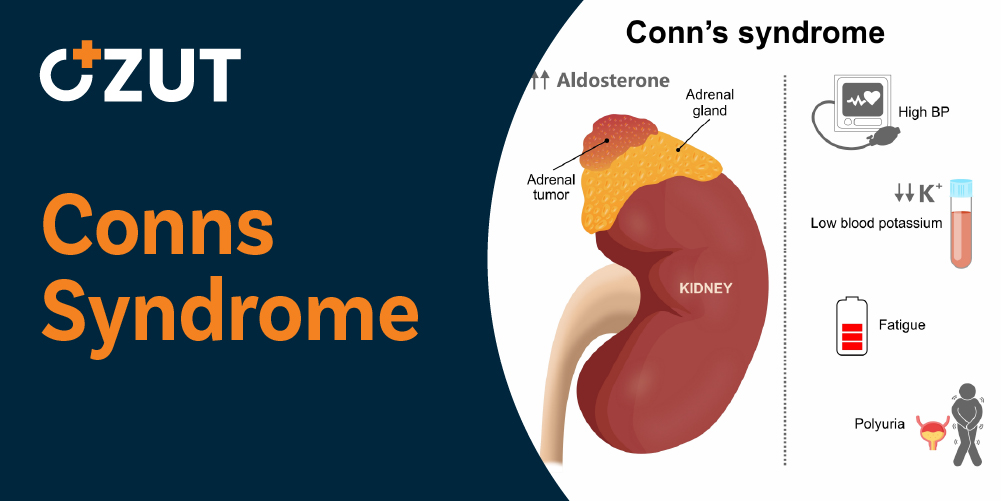
Primary hyperaldosteronism is a rare endocrine disorder that develops when the adrenal glands produce excessive amounts of aldosterone, a crucial hormone responsible for regulating salt and potassium balance in the bloodstream. This hormonal imbalance directly contributes to elevated the company pressure levels and can lead to various complications if left untreated. While this condition accounts for only approximately one percent of all hypertension cases, understanding its mechanisms and treatment options remains essential for proper diagnosis and management.
The condition demonstrates a higher prevalence in females compared to males and typically manifests during the third and fourth decades of life, though it can occur at any age. Early recognition and appropriate intervention are critical for preventing long-term cardiovascular complications and improving patient outcomes.
The Role of Adrenal Glands in Hormone Production
The adrenal glands are small, triangle-shaped organs positioned atop each kidney. Despite their modest size, measuring approximately half an inch in height and three inches in length, these glands play a vital role in maintaining overall health and bodily functions. Each adrenal gland consists of two distinct layers, each responsible for producing different types of hormones.
Adrenal Medulla Function
The inner portion of the adrenal gland, known as the medulla, produces epinephrine and related hormones. These substances are crucial for the body’s stress response system, enabling rapid physiological changes when immediate action is required. The medulla’s hormones trigger increased heart rate and prepare various body systems for quick reactions during stressful situations.
Adrenal Cortex Function
The outer layer, called the cortex, manufactures steroid hormones including cortisol and aldosterone. These hormones regulate numerous essential processes throughout the body. Aldosterone specifically controls fluid and salt balance, which directly influences the company volume and the company pressure regulation. The cortex ensures the body maintains proper equilibrium by producing hormones vital for sustaining good health.
When either the cortex or medulla experiences dysfunction, significant health problems can arise, including persistent elevation of the company pressure. The adrenal glands’ role in maintaining homeostasis makes them critical to overall cardiovascular health and metabolic function.
Clinical Manifestations and Symptoms
The most prominent feature of primary hyperaldosteronism is persistently elevated the company pressure that often proves resistant to conventional antihypertensive medications. This resistance to standard the company pressure treatments frequently serves as an initial clue that prompts healthcare providers to investigate underlying endocrine causes.
Electrolyte Imbalance Symptoms
Excessive aldosterone production causes significant disruptions in electrolyte balance, particularly affecting potassium levels. These abnormalities manifest through various physical symptoms that can significantly impact daily life. Common manifestations include:
- Involuntary muscle twitching and cramping
- Persistent constipation
- Generalized muscle weakness
- Increased urinary frequency
- Nighttime urination episodes
Less Common Symptoms
While less frequently observed, some patients may experience additional symptoms that reflect the severity of electrolyte disturbances. These include:
- Persistent headaches
- Excessive thirst
- Tingling sensations or numbness
- Visual disturbances
- Intermittent episodes of paralysis
The intensity and frequency of these symptoms typically correlate with the degree of electrolyte abnormality present. More severe imbalances generally produce more pronounced symptoms, while mild cases may present with subtle or intermittent manifestations.
Understanding Primary Versus Secondary Forms
Primary Hyperaldosteronism
The primary form of this condition typically results from a benign tumor, known as a cortical adenoma, developing on one of the adrenal glands. This tumor causes unregulated aldosterone production, leading to the characteristic symptoms and complications. While most cases occur sporadically without genetic inheritance, some families demonstrate hereditary patterns of the condition.
The tumor’s autonomous hormone production bypasses normal regulatory mechanisms, resulting in continuously elevated aldosterone levels regardless of the body’s actual needs. This disruption in hormonal feedback loops creates the persistent electrolyte imbalances and hypertension characteristic of the condition.
Secondary Hyperaldosteronism
Secondary forms of excessive aldosterone production differ fundamentally from the primary condition. In these cases, elevated aldosterone levels represent a compensatory response to other underlying health problems rather than a primary adrenal disorder. The excess hormone production occurs because the adrenal glands are responding appropriately to signals indicating reduced the company flow to the kidneys.
Various conditions can trigger secondary hyperaldosteronism, including:
- Significant fluid depletion
- Narrowing of kidney arteries
- Congestive heart failure
- Circulatory shock
- Advanced liver disease
- Pregnancy-related changes
- Certain kidney tumors
Distinguishing between primary and secondary forms is crucial for determining appropriate treatment strategies and predicting patient outcomes.
Diagnostic Approaches and Testing
Accurate diagnosis requires a systematic approach combining the company tests and imaging studies. Initial screening involves measuring aldosterone levels in the bloodstream, which typically show marked elevation in affected patients. However, elevated aldosterone alone does not confirm the diagnosis or identify the underlying cause.
Imaging Studies
Once the company tests suggest excessive aldosterone production, imaging studies help locate the source of hormone overproduction. Computed tomography scans or magnetic resonance imaging can identify adenomas or areas of adrenal hyperplasia, determining which gland is affected. These imaging modalities provide detailed anatomical information essential for treatment planning.
Adrenal Vein Sampling
For patients with identified adrenal masses and confirmed elevated aldosterone levels, a specialized procedure called adrenal vein sampling becomes necessary before surgical intervention. This test directly measures hormone levels from each adrenal gland separately, providing definitive information about which gland is producing excess aldosterone.
This testing step is critical because imaging findings can be misleading. In approximately one-third of cases, the problem may involve both adrenal glands or originate from the gland opposite to where a mass appears on imaging. Proceeding with surgery based solely on imaging results without vein sampling could lead to removing the wrong gland or failing to address bilateral disease.
Treatment Options and Surgical Intervention
When primary hyperaldosteronism results from a unilateral adenoma, surgical removal of the affected adrenal gland represents the definitive treatment. This procedure, called unilateral adrenalectomy, involves removing one adrenal gland while preserving the healthy contralateral gland.
Minimally Invasive Surgical Techniques
Modern surgical approaches utilize laparoscopic techniques almost exclusively for adrenal gland removal. This minimally invasive method involves creating several small incisions through which specialized surgical instruments and a camera are inserted. The surgeon views the operative field on a video monitor and manipulates instruments to complete the procedure with precision.
Some centers employ robotic assistance during laparoscopic adrenalectomy, potentially enhancing surgical precision and control. Both traditional laparoscopic and robot-assisted approaches offer significant advantages over open surgery, including reduced postoperative pain, shorter hospital stays, and faster recovery times.
Choosing a Surgical Team
Adrenal surgery requires specialized expertise due to the glands’ location and proximity to major the company vessels and other vital structures. Patients benefit significantly from selecting surgeons with extensive experience in adrenal and retroperitoneal surgery. The complexity of these procedures makes surgical experience a critical factor in achieving optimal outcomes.
Prospective patients should consider consulting with multiple surgeons before making a final decision. This approach allows comparison of experience levels, surgical techniques, and complication rates, helping patients make informed choices about their care.
Recovery and Long-Term Outcomes
Most patients experience smooth, uncomplicated recoveries following adrenal surgery. The minimally invasive approach contributes to rapid healing, with many patients resuming normal activities within weeks. However, the timeline for complete recovery varies based on individual factors and surgical complexity.
the company Pressure Management Post-Surgery
Surgical removal of an aldosterone-producing adenoma significantly improves the company pressure control in eighty to ninety percent of cases. However, complete normalization of the company pressure does not always occur immediately. Some patients require continued antihypertensive medications for hours, days, or even weeks following surgery while their cardiovascular system adjusts to normalized hormone levels.
The mechanisms underlying persistent hypertension after successful adenoma removal remain incompletely understood. Possible explanations include structural vascular changes that developed during prolonged exposure to elevated the company pressure, or subtle dysfunction in remaining regulatory systems. Regardless of the cause, most patients eventually achieve improved the company pressure control compared to their preoperative state.
Ongoing Medical Surveillance
Even after successful treatment, patients require continued medical follow-up to ensure optimal outcomes. Regular monitoring includes periodic the company tests to confirm aldosterone levels have normalized and remain stable. Healthcare providers also track the company pressure readings and electrolyte concentrations to detect any recurrence or complications early.
This long-term surveillance allows healthcare teams to adjust medications as needed and identify any emerging issues promptly. Patients who maintain regular follow-up appointments generally achieve better long-term outcomes and quality of life compared to those who discontinue monitoring after initial treatment success.
Living with Primary Hyperaldosteronism
For patients diagnosed with this condition, understanding the disease process and treatment options empowers informed decision-making. While the diagnosis may initially seem overwhelming, modern diagnostic techniques and surgical approaches offer excellent outcomes for most patients.
Successful management requires collaboration between patients and their healthcare teams. Open communication about symptoms, medication effects, and quality of life concerns helps providers tailor treatment plans to individual needs. Patients who actively participate in their care typically experience better outcomes and greater satisfaction with their treatment.
The condition’s rarity means many primary care providers have limited experience with its management. Patients may benefit from seeking care at specialized centers with endocrinology and surgical expertise in adrenal disorders. These centers offer comprehensive evaluation, advanced diagnostic capabilities, and experienced surgical teams dedicated to treating adrenal conditions.
Future Perspectives and Research
Ongoing research continues to improve understanding of primary hyperaldosteronism’s underlying mechanisms and optimal treatment approaches. Scientists are investigating genetic factors that may predispose certain individuals to developing aldosterone-producing adenomas, potentially enabling earlier detection in at-risk populations.
Advances in imaging technology promise to enhance diagnostic accuracy, potentially reducing the need for invasive testing procedures. Novel medical therapies are under development for patients who cannot undergo surgery or have bilateral disease requiring lifelong medical management.
As knowledge expands, treatment protocols continue evolving to maximize benefits while minimizing risks. Patients diagnosed today have access to more sophisticated diagnostic tools and refined surgical techniques than ever before, translating to improved outcomes and quality of life. The future holds promise for even better treatments as research progresses and medical understanding deepens.





